
Figure 1: Left parotideal lesion gradually increased in 6 months

Merih Onal* Gultekin Ovet Esra Yılmaz Necat Alatas
Department of Otorhinolaryngology, Konya Education and Training Hospital, Konya, Turkey*Corresponding author: Merih Onal, Department of Otorhinolaryngology, Konya Education and Training Hospital, Konya, Turkey, E-mail: drmerihonal@gmail.com
Malignancies arising from putative natural killer (NK) cells are recently recognized distinct lymphoma subtype. Clinically, these lymphomas present most commonly as destructive lesions in the nasal cavity and other midline facial structures. Lymphomas of putative NK cells occur primarily in nonnasal areas including skin, gastrointestinal tract, salivary gland, testis and muscle. The molecular mechanisms leading to malignant transformation of NK cells remain undefined but one of the pathogenetic association is EBV infection. Lymphoma infiltration is seen with prominent necrosis and vascular destruction. Although the clinicopathological features of NK cell lymphomas are well defined, the optimal therapy and treatment outcomes are unclear. Unfortunately, the treatment of NK cell lymphoma has been unsatisfactory. Conventional chemotheraphy treatment regimens have resulted in very poor complete remission rates and long-term survival. Here we presented an unusual case of NK cell lymphoma involving the parotid gland.
Extranodal NK/T-Cell lymphoma, nasal type (NKTLN) is a disease that mainly affects the nasal cavity and paranasal sinuses [1]. According to the World Health Organization classification, the term ‘nasal type’ used for diseases that arise in the nasal cavity and extranasal sites [2]. Nasal/ nasopharyngeal localization represents 75% of the cases [3]. Extra-nasal affected sites are skin, larynx, testes, gastrointestinal tract and kidneys [1]. Salivary gland lymphomas constitute 2–5% of all salivary gland neoplasms [4]. Most primary salivary gland lymphomas originated from B cell lineage [5]. We report here a rare case, NK/T-Cell lymphoma in parotid gland which was represented with an excellent outcome as a result of chemotherapy.
A 14-year-old girl referred to our clinic with a 2 cm mass which was located in the parotid gland region. The swelling had appeared two months ago with discoloration of overlying skin. Oral, nasopharyngeal and laryngeal examination was normal. Total excision of the lesion and biopsy was recommended but her family did not accept the surgery for diagnosis. After six months later, the patient came with a huge lesion extending into posterior cervical region which was gradually increased in size from about 2 × 2 cm to 10 × 10 cm (Figure 1). The lesion was necrotic and crusty. In magnetic resonance imaging, a 9-cm cystic and necrotic mass was observed which was originating from the deep lobe of the parotid gland and infiltrating all of the parotid and the overlying skin (Figures 2 and 3). First biopsy was reported as ‘chronic inflammation’. Second biopsy was taken from deeper part. Based on histomorphology, diagnosis of NK/T-Cell lymphoma- nasal type was made. After this diagnosis patient was referred to Oncology Department. She underwent systemic imaging studies for systemic involvement and no any dissemination of the disease was encountered. The patient started on methotrexate, ifosfamide, cyclophosphamide, vincristine, mesna, etoposide and cytarabine chemotherapy by oncologist. The response to the treatment was excellent, at the sixth month of the therapy, the lesion was disapperared almost totally (Figure 4).
Figure 1: Left parotideal lesion gradually increased in 6 months
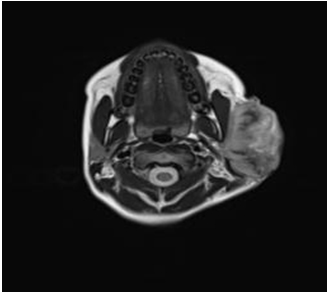
Figure 2: Axial section of the parotid lymphoma
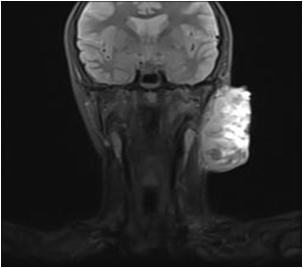
Figure 3: Coronal section of the parotid lymphoma

Figure 4: At the sixth month of treatment, the tumor disappeared
Extranodal non-Hodgkin’s lymphomas (NHL) of the head and neck affect Waldeyer’s ring, nasopharynx, nasal cavity, paranasal sinuses, thyroid gland, orbit, and salivary glands [6]. Primary parotid lymphomas account for 0.87% of all NHL cases and 4–5% of all extranodal NHLs [7]. And they may arise from intraparotid lymph nodes or gland itself [8]. Males in the fifth decade are predominantly affected patient group [9]. Our patient is a girl and she is 14 years of age. The majority of all nonHodgkin parotid lymphomas originated from B-cell lineage including low grade B cell lymphoma of MALT (Mucosa-associated lymphoid tissue), follicular lymphoma and DLBCL (Diffuse Large B Cell Lymphoma) [10]. Lymphomas derived from NK cells are rarely encountered and associated with Epstein-Barr virus (EBV). Nasal NK cell lymphoma is much more common in Asians so a racial predisposition may have a role in the pathogenesis [6]. Most of the salivary gland lymphoma cases present with painless, firm swelling in the gland region [5]. As the biopsy is postponed, significant increase seen in necrosis [1]. In our patient, the disease was diagnosed as NK/T cell lymphoma in the second biopsy. Thus, the earlier biopsy is performed, the greater chance to obtain diagnostic tissue sample [11]. Diagnosis of NHL requires evaluation of any other systemic involvement to decide on the therapy. There was no dissemination of the disease in our patient [5]. Currently, there is no standardized treatment protocol for NKTLN [11]. The treatment based on chemotherapy along with locoregional radiotherapy, but the prognosis is poor [12]. Unfortunately, patients with extranodal NK/T-cell lymphoma have a cumulative 5-year survival around 40% [13]. But our patient’s prognosis seems to be great for the present.
Parotid gland lymphomas clinically indistinguishable from other benign or malignant lesions. Definitive diagnosis may be postponed by the patient with being late to seek a medical advice or by the doctor with non-helpfull imaging modalities [5]. The extranasal disease has a poor clinical outcome hence new treatment modalities should be considered [3].
Download Provisional PDF Here
Article Type: Case Report
Citation: Onal M, Ovet G, Yılmaz E, Alatas N (2015) NK-Cell Lymphoma Involving the Parotid Gland: A Rare Case. J Surg Open Access 1(2): doi http://dx.doi. org/10.16966/2470-0991.107
Copyright: © 2015 Onal M, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Publication history:
All Sci Forschen Journals are Open Access